Common Foot and Ankle Injuries and Associated Movement Deficiencies
The human body is susceptible to movement dysfunctions and neuromusculo skeletal imbalances. Some causes may include repetitive movements, overuse, sedentary living, and improper movement techniques. These dysfunctions in turn lead to many of the common injuries seen in an active population. The foot and ankle complex may greatly influence the entire human movement system. This region represents the platform from which our base of support is derived and is the main contact point between the ground and the body. As such, it must withstand a high amount of contact force (ground reaction force) with each step taken because it is closest to the impact site (foot strike). As the body is an interconnected chain (kinetic chain), compensation or dysfunction in one region such as the foot and ankle may lead to dysfunctions in other areas of the body.
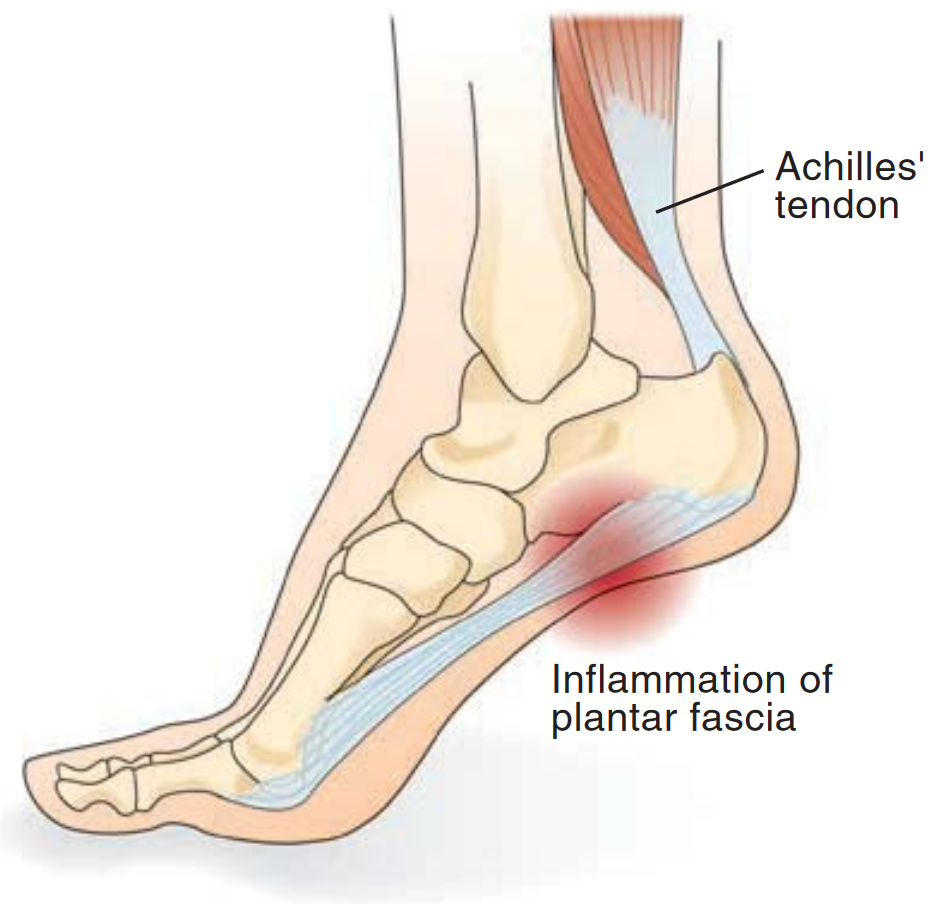
Plantar Fasciitis
The plantar fascia is a thick, fibrous band of tissue that runs from the calcaneus and fans out to insert on the metatarsal heads to support the longitudinal arch of the foot. An inflamed and irritated plantar fascia can be very painful. Plantar fasciitis is a common cause of heel pain, and most patients report pain in the heel region, particularly after getting out of bed in the morning or after sitting for extended periods. Lack of ankle dorsiflexion has been associated with plantar fasciitis, as has a pronated foot type. Increased body mass index in a nonathletic population has also been indicated as a predisposing factor. However, there is not strong evidence to associate foot type or first metatarsophalangeal joint motion with plantar fasciitis. Stretching of the calf or plantar fascia appears to provide short-term pain relief and improvements in dorsi flexion range of motion.
Achilles’ Tendinopathy
The gastrocnemius complex, which consists of the gastrocnemius and soleus muscles, share a common Achilles’ tendon that inserts on the base of the calcaneus. Tendonitis, or inflammation of this tendon, is a common sports-related injury. Tendonitis, or inflammation of this tendon, is a common sports-related injury. Alternately, if inflammation is not present, but tendinopathy and tissue degeneration are present, it is termed tendinosis. Jumping and running are common causes of Achilles’ tendinopathy. Signs and symptoms may include pain during physical activities or at rest, inflammation, swelling, and thickening of the tendon. A tight Achilles’ tendon (lack of dorsiflexion) and increased rear foot inversion has been associated with Achilles’ tendinopathy. Additionally, runners with Achilles’ tendinopathy demonstrated decreased knee range of motion, and decreased activity in the tibialis anterior, rectus femoris, and gluteus medius muscles in the time before and after heel strike. Eccentric exercise of the tendons appears to treat the condition, but care must be taken to not worsen the injury.
Medial Tibial Stress Syndrome
Medial tibial stress syndrome, which has been called shin splints, is an overuse injury thought to be caused by excessive running or training, poor shoes, type of training surface, or biomechanical factors. Individuals with medial tibial stress syndrome complain of pain and tenderness along the medial tibia, usually in the distal one third. Pain is oft en worst during or aft er activity. Pain is attributed to either irritation of the periosteum or bone stress reaction in the tibia. Increased plantar flexion range of motion, or differences in ankle joint range of motion, and the use of orthotics have been associated with medial tibial stress syndrome. Over pronation has been linked as a risk factor, as has increased passive inversion and eversion range of motion at the ankle, internal and external rotation at the hip, and lack of muscular endurance in the calf. Women and individuals with decreased running or activity experience seem to be more at risk for this injury. There is not evidence to support intensity, distance, training surface, change in shoes, or age of shoes as risk factors.


Ankle Sprains and Chronic Ankle Instability
Ankle sprains are reported to be the most common sports-related injury, but can also result from as something as simple as incorrect foot placement when walking. Lateral ankle sprains are the most common type of sprain, and affect the lateral ankle ligaments, including the anterior talofibular ligament, calcaneofibular ligament, and posterior talofibular ligament. Individuals who experience a lateral ankle sprain are at risk for developing chronic ankle instability. Research has shown that 30 % of first time lateral ankle sprain (LAS) sufferers develop chronic ankle instability. Chronic ankle instability is defined as repetitive episodes of giving way at the ankle, coupled with feelings of instability. CAI is thought to be the result of neural (proprioception, reflexes, muscular reaction time), muscular (strength, power, and endurance), and mechanical mechanisms (ligamentous laxity). Several risk factors for ankle sprain have been identified, including previous sprain and decreased ankle dorsiflexion range of motion. Individuals with increased arch height and women with increased calcaneal eversion range of motion are also at increased risk for ankle sprain. Foot width and type, anatomic alignment, sex, and generalized joint laxity have been proposed as risk factors for ankle sprain, but there is little evidence to support these claims. Although strength is an important consideration in the prevention of ankle sprains, there is also limited conclusive evidence to link muscular weakness to ankle sprain. Evertor muscle weakness does not appear to be a factor in ankle sprain. However, invertor strength deficits may be present in those with chronic ankle instability. It has also been shown that individuals may experience hip weakness aft er an ankle sprain. Additionally, individuals with ankle instability may demonstrate arthrogenic muscle inhibition of the soleus and peroneals.
Foot and Ankle Dysfunction and the Human Movement System Chain Reaction
If the foot excessively externally rotates and/or everts (excessive pronation) during movement, the foot and ankle complex and lower leg will alter motion accordingly as components of the kinetic chain. From a mechanical perspective, foot pronation can lead to tibial rotation and femoral adduction and internal rotation (or knee valgus). Musculature imbalance and tightness is theorized to contribute to this position. Specifically, tightness of the lateral ankle musculature (lateral gastrocnemius, soleus, and peroneals) may influence tibial abduction and rotation, which can influence femoral adduction and internal rotation. If antagonistic muscles (medial gastrocnemius, anterior tibialis, and posterior tibialis) are weak, they may be unable to overcome the valgus joint positioning. This constant valgus position could potentially lead to additional tightness of the short head of the biceps femoris (tibial abduction with concomitant femoral adduction) as well as tightness in the tensor fascia latae (femoral internal rotation). The medial gastrocnemius has been identified as a dynamic stabilizer of the knee and counteracts a knee valgus moment. An electromyography (EMG) study of muscle electrical activity indicated that individuals with pronated feet demonstrated increased EMG amplitude in the tibialis anterior, lateral gastrocnemius, and soleus in some phases of gait, and decreased EMG for the soleus, medial gastrocnemius, and lateral gastrocnemius in others. When arch height was increased via an orthotic insert, increased EMG activity was noted in the vastus medialis and gluteus medius during a single-leg squat and a lateral step-down. It appears that pronation may have an effect on lower extremity muscle activity, and that increasing arch height (decreasing pronation) can alter that muscle activity.
Your feet are the foundation for your entire body. They must be able to properly support your body; allow you to stand, walk, run, and jump; and absorb damaging shock that enters your body every time your heel hits the ground. Every athlete deals with structural defects, many of which start in the feet. Foot imbalance or dysfunction does not always cause pain just in your feet - the pain may transfer to your lower legs, knees, hips or spine instead. As the body is an interconnected chain, compensation or dysfunction in one region such as the foot and ankle may lead to dysfunctions in other areas of the body. For this reason, it becomes a crucial region to assess. Symptoms that are being felt in other regions of the body could potentially be caused by dysfunction at the foot and ankle complex. If not assessed, the symptoms may be addressed, but the cause of those symptoms is not, with reoccurring injury being the result. Eighty percent of people develop some type of foot imbalance by the age of 20, and virtually everyone has foot imbalances by the age of 40. After years of standing, walking, and wearing shoes, the arches of your feet gradually weaken and are not able to provide the necessary support for your body.
Identification of dysfunction is achieved through an integrated assessment process, which includes static posture, transitional movement assessments, dynamic movement assessments, goniometric (range of motion) measurements, and manual muscle testing. The integrated assessment process allows the health and fitness professional to identify range of motion restrictions, muscle weakness or imbalance, and poor movement patterns. Once these deficits are identified, the corrective procedure strategy (eg. Exercise and / or manual therapy) can be developed.

Effects of excessive foot and ankle pronation.
REFERENCES
1. Powers CM. The influence of altered lower-extremity kinematics on patellofemoral joint dysfunction. J Orthop Sports Phys Ther. 2003
2. Sahrmann S. Diagnosis and Treatment of Movement Impairment Syndromes . St. Louis. MO: Mosby; 2002.
3. Bell DR, Padua DA, Clark MA. Muscle strength and flexibility characteristics of people displaying excessive medial knee displacement. Arch Physical Med Rehabil. 2008
4. Geraci MC, Brown W. Evidence-based treatment of hip and pelvic injuries in runners. Phys Med Rehabil Clin N Am. 2005
5. Beckman SM, Buchanan TS. Ankle inversion injury and hyper-mobility: effect on hip and ankle muscle electromyography onset latency. Arch Physical Med Rehabil. 1995
6. Irving DB, Cook JL, Menz HB. Factors associated with chronic plantar heel pain: a systematic review. J Sci Med Sport. 2006