Common Knee Injuries and Associated Movement Deficiencies
Lower extremity injuries account for more than 50% of injuries in college and high school athletes, and among lower extremity injuries, the knee is one of the most commonly injured regions of the body. Researchers have estimated health care costs to be approximately $2.5 billion annually for anterior cruciate ligament (ACL) injuries. The knee is apart of a kinetic chain that is greatly affected by the linked segments from the proximal and distal joints. The foot and ankle and the lumbo-pelvic-hip complex play a major role in knee impairment, as the structures that help to form the ankle and hip joints make up the knee joint. This region is a prime example of how alterations in other joints within the human movement system can dramatically affect the movement and increase the stress and injury capacity of another joint, which leads to knee impairments.
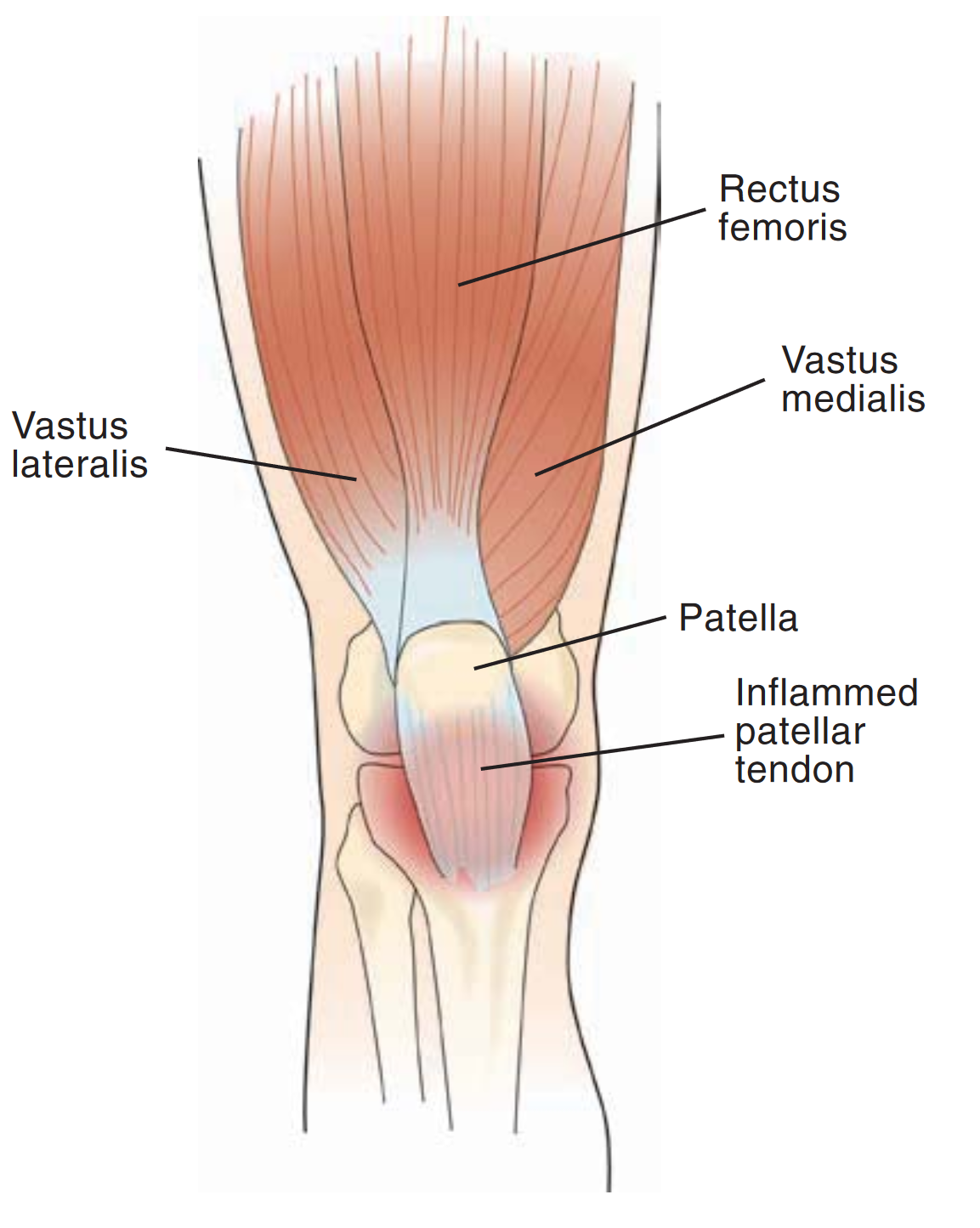
Patellar Tendinopathy (Jumper’s Knee)
Patellar tendinopathy is a common overuse injury. It occurs when an individual places repeated stress on the patellar tendon. The stress results in tiny tears in the tendon, which may cause necrotic degenerative change or inflammation in the tendon and pain. Patellar tendinopathy is a ninjury common with, but not limited to, athletes, particularly those participating in jumping sports such as basketball, volleyball, or high or long jumping. Risk factors for patellar tendinopathy include the following:
· Knee valgus and varus
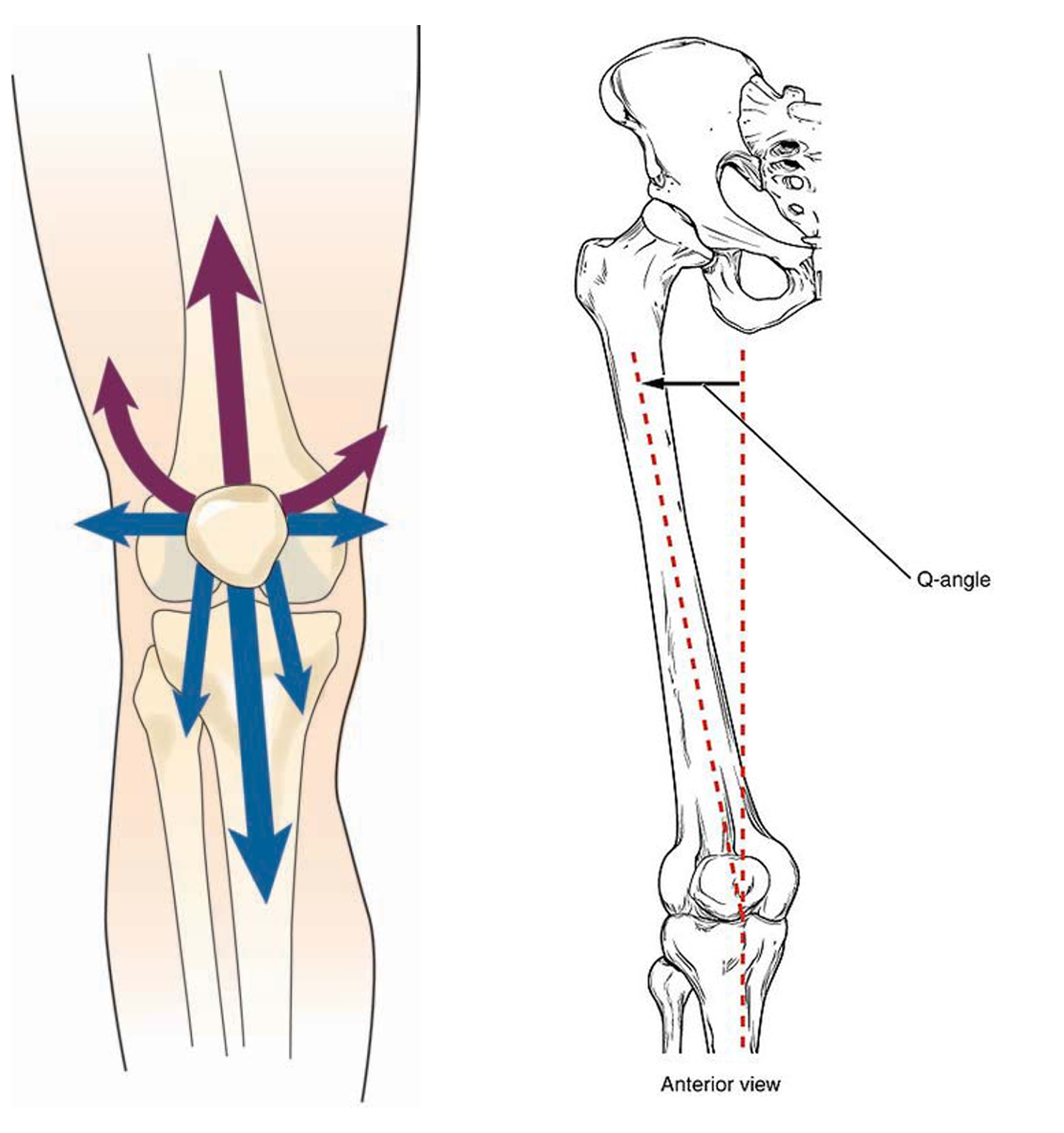
· An increased Q angle
· Poor quadriceps and hamstring complex flexibility
· Poor eccentric deceleration capabilities
· Overtraining and playing on hard surfaces
Patellofemoral Syndrome
One of the most commonly accepted causes of patellofemoral syndrome (PFS) is abnormal tracking of the patella within the femoral trochlea. When the patella is not properly aligned within the femoral trochlea, the stress per unit area on the patellar cartilage increases owing to a smaller contact area between the patella and the trochlea. Abnormal tracking of the patella may be attributable to static (i.e., increased Q-angle) or dynamic lower-extremity malalignment (i.e., increased femoral rotation, adduction, and knee valgus), altered muscle activation of surrounding knee musculature, decreased strength of the hip musculature, or various combinations.
Patellofemoral Syndrome
Anterior Cruciate Ligament (ACL) Injury
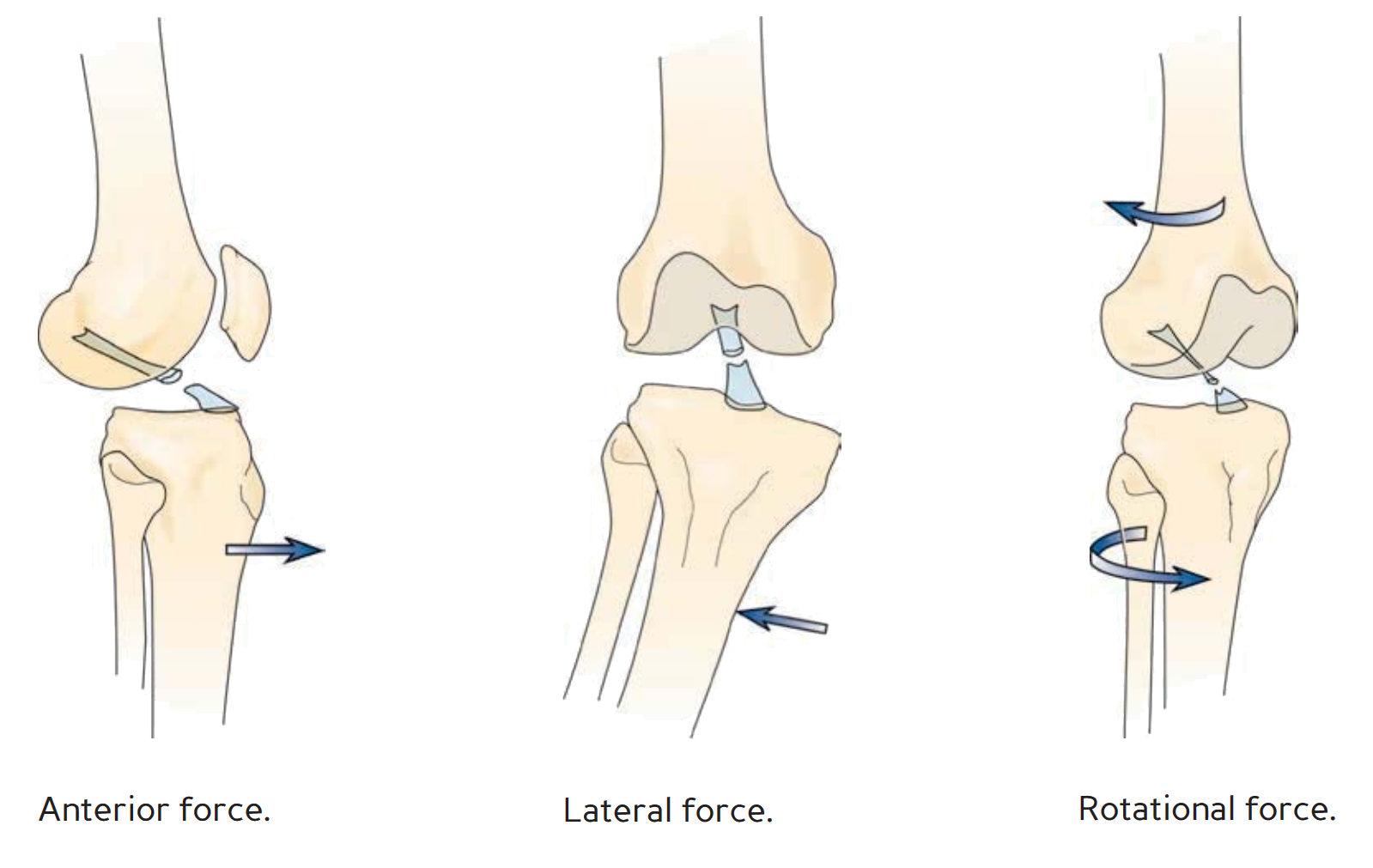
Beyond the common injuries indicated that are more chronic in onset, recent studies also indicate that altered lower extremity neuromusculo-skeletal control imbalances can increase the risk of acute injures such as ACL ruptures. Specifically, peak landing forces were significantly predicted by valgus torques at the knee, women demonstrated decreased relative knee flexor torque during landing compared with men, and women had greater side-to-side differences in normalized hamstring complex peak torque. Insufficient neuromusculo-skeletal control of lower limb biomechanics, particularly frontal plane control of the knee joint, leads to high risk patterns in female athletes during execution of common, albeit potentially hazardous, movements. These sex differences are evident during landing and cutting in soccer and basketball athletes. Female athletes also have significant differences between their dominant and non dominant sides in maximum valgus knee angle. These differences in valgus measures (ligament dominance) and limb to limb asymmetries (leg dominance) reflect neuromusculo-skeletal control deficits that may be indicative of decreased dynamic knee joint control in female athletes.
Anterior Cruciate Ligament (ACL) Injury
Subsequent studies systematically evaluated more proximal neuromusculo-skeletal control deficits at the hip and trunk to help determine potential contributing mechanisms to high-risk knee mechanics during landing. When performing single leg landing tasks, female athletes demonstrated increased trunk flexion and lateral tilt range of motion. In addition to greater knee abduction angles, female athletes had increased hip frontal plane excursion compared with men during both types of landings. The increased hip adduction motion seen in the frontal plane during athletic activities likely contributes to the dynamic valgus knee position that may place the athlete at increased risk of knee injury. Neuromusculoskeletal control imbalances are often evident in adolescent female athletes, which include ligament dominance (decreased lower extremity frontal plane stability), quadriceps dominance (decreased relative strength or recruitment of the posterior chain musculature), and leg dominance (limb-to-limb asymmetries in neuromusculo-skeletal control or muscle recruitment).
The first step in developing a corrective exercise strategy for knee impairments is an integrated assessment process. On the basis of the information obtained from these assessments collectively, the neuromusculo-skeletal control deficits can be identified for targeted treatments.
REFERENCES
1. Hootman JM, Dick R, Agel J. Epidemiology of collegiate injuries for 15 sports: summary and recommendations for injury prevention initiatives. J Athl Train. 2007
2. Fernandez WG, Yard EE, Comstock RD. Epidemiology of lower extremity injuries among U.S. high school athletes. Acad Emerg Med. 2007
3. Garrick JG, Requa RK. ACL injuries in men and women—How common are they? In: Griffi n LY, ed. Prevention of Noncontact ACL Injuries . Rosemont, IL: American Academy of Orthopaedic Surgeons; 2001.
4. Greslamer RP, Klein JR. Th e biomechanics of the patellofemoral joint. J Orthop Sports Phys Th er. 1998